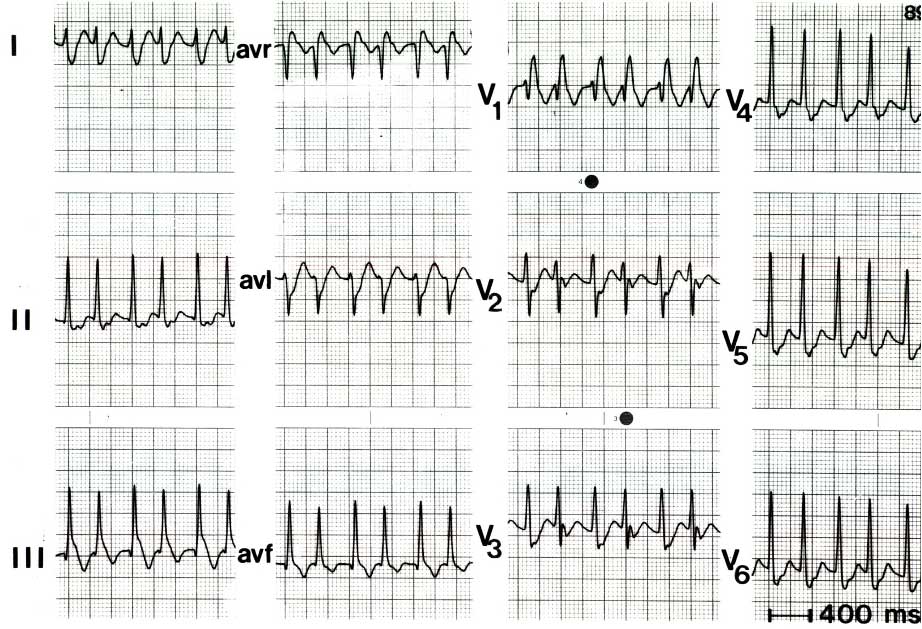
Male patient, 42 years old, who consults for paroxysmal episodes of tachycardia which have worsened in recent months. They do not give way with vagal maneuvers, they have never collapsed, the tachycardia lasts more than 3 hours. He arrives today at the emergency department, with BP of 100/60, pulse of 180 BPM, and associated precordial tightness. 12-derivations ECG taken.
What would your diagnosis be?
SVT com RBBB devido ao fenômeno de Ashman (bloqueio da Fase 3)
Resposta correta: 5. Todas estão corretas
TMC usando uma rota acessória
Resposta correta: 5. Todas estão corretas
Dissociação longitudinal do Nodo AV
Resposta correta: 5. Todas estão corretas
Via acessória póstero-septal direita
Resposta correta: 5. Todas estão corretas
Todas las anteriores son correctas
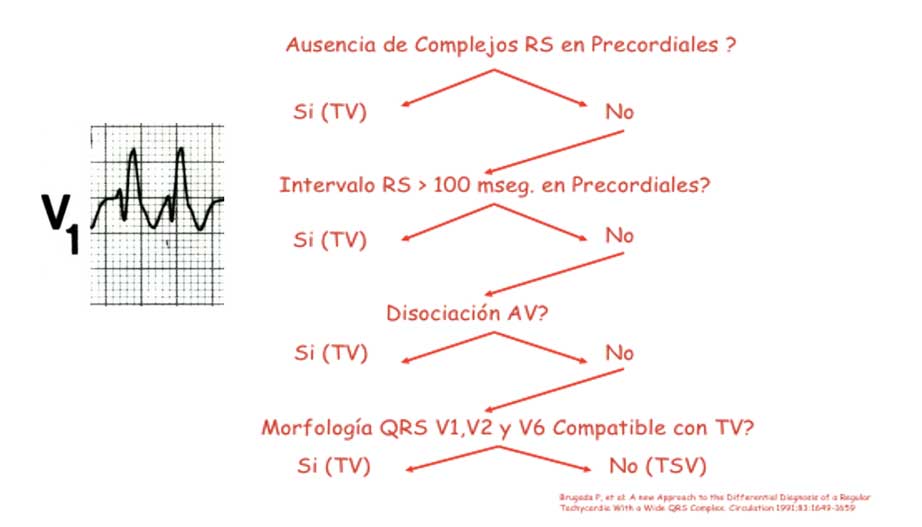
Brugada algorithm for TCA
Explain each point of the Brugada algorithm shown in the images
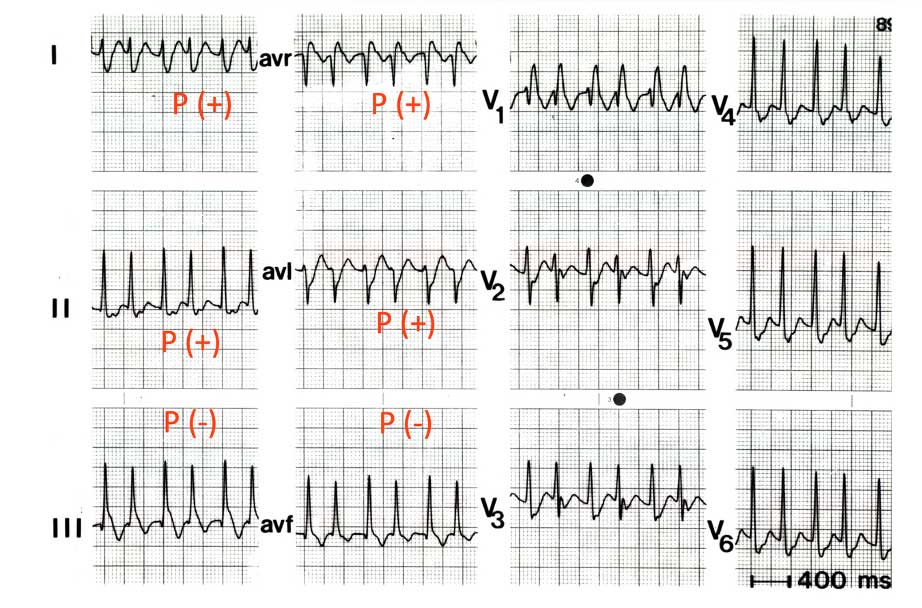
1. Absence of RS complexes in the precordials means that all QRS from V1 to V6 are positive (pure R) or negative (QS), also called positive concordance and negative concordance, respectively. Having RS complexes in the precordials means that there is at least one QRS complex with positive and negative polarity, for example in V1 the complex is rSR’, in V2 the complex is RS.
2. If there are RS complexes in any of the precordials, their duration must be measured, since if it has a duration >100 ms it points to the ventricular origin of the tachycardia, in this example the duration of the QRS in V2 is 60 ms.
3. AV dissociation (presence of P waves that are not related to the QRS complexes) confirms a ventricular origin of the tachycardia, in this electrocardiogram all the P waves are found after the QRS, guiding a retrograde activation of the atria after the ventricular depolarization.
4. When the morphology of the QRS in the precordials corresponds to right branch block of the bundle of his, the morphology that guides the supraventricular origin is the classic rSR’ morphology in V1, taking into account that the first r must be smaller than the second R and that in V6 the positive portion of the QRS must be greater than the negative portion (R/S >1)
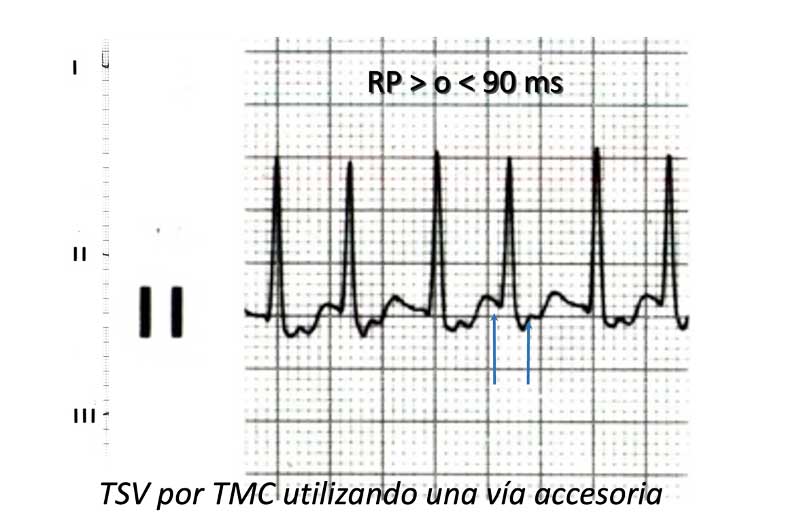
How is the PR?
The RP should be measured from the beginning of the QRS to the beginning of the next P wave. If it has a duration shorter than the PR (start of the P wave to the beginning of the next QRS), it means that the RP is short (RP<PR ). Having a short RP there are two possibilities, that it has a duration ≥90 ms or <90 ms, in the first option it would be a tachycardia due to circular movement mediated through an accessory pathway, and in the second option it would be a re-entry of the common variety AV node. In this ECG the RP lasts approximately 120 ms.
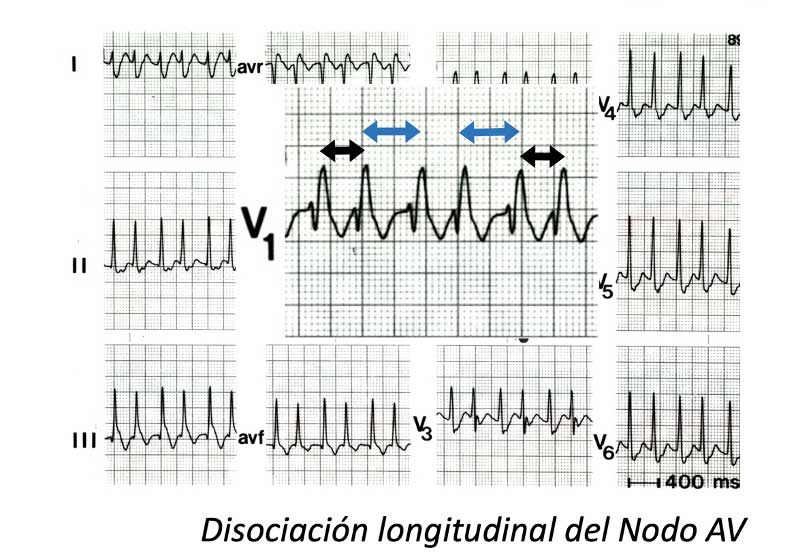
Why does it vary in RR?
The RR varies because there is a longitudinal dissociation of the AV node (which means that it leads through both pathways), once it leads anterogradely through the fast pathway and again through the slow pathway, generating shorter and longer RRs, respectively.
Location of the accessory pathway
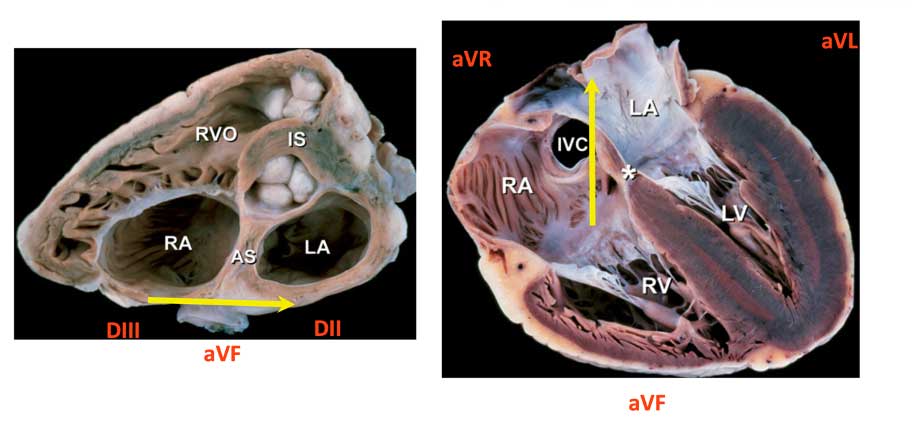
If we take into account that the P wave is retrograde, the origin of the accessory pathway can be identified, since if the P wave is positive in a derivation it means that it is approaching it, and if, on the contrary, it is negative, it means that it is moving away from this derivation.
In this electrocardiogram the accessory pathway is located in the right posteroseptal region: it is located in the posterior (inferior) wall and that is why the P wave is positive in aVL and aVR; It comes from the right side because the P wave is positive in DI and negative in DIII.
Case diagnosis
- ED with RBBB (Aberrancy)
- RP>90 msg = TMC (accessory pathway)
- Regularly variable RR
- Longitudinal dissociation of the AV Node
- Location: Right PS pathway: P(-) DIII and P (+) aVR-aVL and P (+) in DII
Autor:

Prof. Mauricio Duque R. MD, FHRS, FACC. FESC.
Internista-Cardiólogo-Electrofisiólogo
Profesor Titular Universidad CES
Profesor Emérito Universidad CES
Jefe de postgrado de Electrofisiología Universidad CES.